21 YEARS OLD FEMALE WITH VIRAL PNEUMONIA SECONDARY TO COVID-19
"This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs".
This E log book also reflects my patient-centered online learning portfolio and your valuable comments on comment box is welcome.
MEDICINE CASE DISCUSSION:
I've been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
VIEW OF THE CASE :
A 21 years old female, student by occupation, hailing from Nalgonda came to OPD with chief complaints of fever since 7 days and shortness of breathe since 3 days, cough, fever, vomitings and motions since 3 days.
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 3 days back
later she developed shortness of breathe since 3 days which is insidious in onset, progressive with Grade I to II, increased on exertion, releived on rest.
There is orthopnoea and No PND
She is tested RAPID ANTIGEN TEST for COVID-19 POSITIVE from the time of admission.
She complains of cough since 3 days with expectoration,mucoid, non foul smelling,
History of fever since 3 days which is insidious in onset, continuous, high grade associated with chills and rigor.
History of vomitings since 3 days.
History of passing loose stoolssince 3 days(5-6 episodes per day)
There is decreased urine output since 3 days.
No history of chest pain, wheeze, hemoptysis, loss of weight
PAST HISTORY:
She is a known case of HYPERTENSION since 1 year
Abdominal distension since 6 months.
She got an attack of epilepsy 2 months back
No history of Diabetes, CAD, Asthma, Tuberculosis
TREATMENT HISTORY:
She has been taking medications TAB. NICARDIA 10mg and ARTAMINE 40 mg for hypertension since 1 year
History of kidney biopsy in 2016
She was on dialysis treatment since 1 year(every 15 days for 6 months and every alternate day since past 6 months)
PERSONAL HISTORY:
Appetite- loss of appetite
Diet- mixed
Bowel habits- passing loose stools
Bladder habits- decreased urine output
Sleep- adequate
Addictions- no addictions
Allergies- no allergies
FAMILY HISTORY:
Insignificant
GENERAL EXAMINATION:
Conscious, coherent and cooperative
Well oriented to time, place and person
Moderately built and moderately nourished
Pallor- PALLOR PRESENT
Icterus- No icterus
Cyanosis- No Cyanosis
Clubbing- No clubbing
Generalised lymphadenopathy- No generalised lymphadenopathy
Pedal edema- BILATERAL PEDAL EDEMA
Malnutrition- No
Dehydration- No
VITALS:
Temperature - 98.9°F
Pulse rate- 90 bpm
Respiratory Rate- 30 cycles per minute
Blood Pressure- 120/80 mm of Hg
SpO2- 85% at room air
GRBS- 172 mg%


SYSTEMIC EXAMINATION:
CARDIOVASCULAR SYSTEM- S1 and S2 heart sounds heard, no murmers
RESPIRATORY SYSTEM- Bilateral air entry present with vesicular breath sounds and no added sounds
CENTRAL NERVOUS SYSTEM- intact
ABDOMEN- no organomegaly
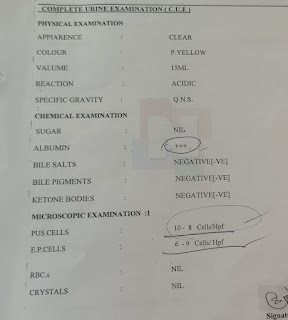
INVESTIGATIONS:
LFT:
Total bilirubin : 2.14 mg/dl
Direct Bilirubin: 0.81 mg/dl
Alkaline phosphate: 154 IU/L
Total Proteins: 5.2gm/dl
Albumin : 2.7gm/dl



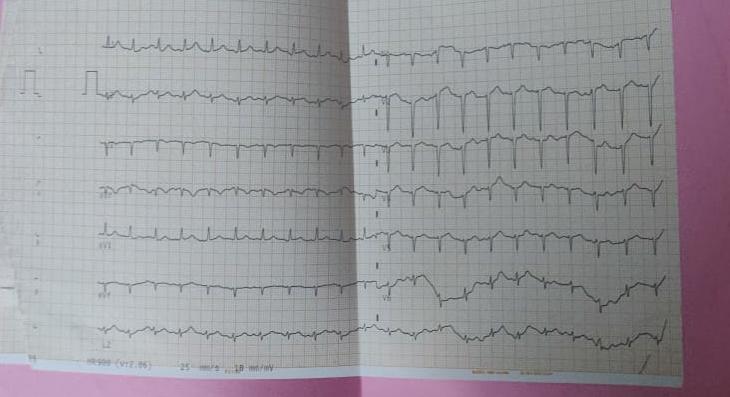
ECG-

DIAGNOSIS:
CKD ON MAINTENANCE HEMO DIALYSIS WITH HYPERTENSION WITH COVID-19 POSITIVE
TREATMENT :
- INJ. AUGMENTIN 25mg IV BD
- INJ. METROGYL 400mg TID/PO
- INJ. PAN 40mg IV OD
- INJ. ERYTHROPOIETIN 4000IU S/C TWICE WEEKLY
- TAB. NODOSIS 500mg BD
- TAB. ZOFER 4mg BD
- TAB. SPOROLAC TID
- SYP. ASCORIL 2 TSP TID
- TEPID SPONGING
- TAB. PCM 650mg (SOS)
- O2 INHALATION WITH FACEMASK at 4L/MIN
- INJ. LASIX 40mg BD
- MONITOR VITALS
- GRBS MONITORING 6TH HOURLY
- TAB. BUSCOPAN SOS
- INJ. LEVOFLOX 500mg IV/OD
ONE BLOOD TRANSFUSION IS DONE I/V/O SEVERE ANEMIA DURING HEMODIALYSIS
Patient died on 3rd day of hospitalization at 2:21pm.
DEATH SUMMARY:
Patient is a known case of CKD and is on MAINTENANCE HEMODIALYSIS since 1 year. Patient was complaining of shortness of breathe, cough, fever, vomitings and loose stools since 3 days. From the time of admission RAPID ANTIGEN for COVID-19 was POSITIVE. Patient was placed on appropriate antibiotics, O2 Inhalations, Nebulization and one blood transfusion was done I/V/O SEVERE ANEMIA during hemodialysis. Patient started complaining of SEVERE SHORTNESS OF BREATHE and is not releived with nebulization. Patient had SUDDEN CARDIAC ARREST on 03.05.2021 at 1:40pm. Pulse was absent and not responsive. Immediate intubation and CPR was started according to 2015 AHA guidelines. Inspite of our efforts, patient couldn't be revived and declared dead at 2:21pm on 03.05.2021 after confirming no electrical activity on ECG(flat line).
Immediate cause: SUDDEN CARDIAC ARREST
Antecedent cause: CKD ON MHD WITH VIRAL PNEUMONIA SECONDARY TO COVID-19
CPR:





Comments
Post a Comment