65 YEARS OLD MALE WITH VIRAL PNEUMONIA SECONDARY TO COVID-19.
"This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs".
This E log book also reflects my patient-centered online learning portfolio and your valuable comments on comment box is welcome.
KASTURI VIJAY KUMAR
8TH SEMESTER, ROLL NO : 56
MEDICINE CASE DISCUSSION:
I've been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
VIEW OF THE CASE :
A 65 years old male hailing from Miriyalaguda came to OPD with chief complaints of fever since 7 days and shortness of breathe since 3 days with loss of appetite and weakness and altered sensorium since 2 days.
History of present illness:
The patient was apparently asymptomatic 7 days back, and then he developed fever which was insidious in onset, high grade, intermittent, not associated with chills and rigor and subsided with medication(Paracetamol) given by RMP. And he got RAPID ANTIGEN TEST for COVID-19 which is tested NEGATIVE done on 14.05.2021 (reports are not available).
Later he developed shortness of breathe 3 days back which is of Grade-II to III, aggravated on exertion. There is no orthopnoea( discomfort when breathing while lying down) and PND ( paroxysmal nocturnal dyspnoea).
There is altered sensorium ( GCS - E2V2M5) since 2 days.
He complaints of scrotal swelling since 10 years.
He also complaints of loss of appetite and weakness.
There is no history of cough and cold.
HRCT( High Resonance CT) was done on 18.05.2021 which reported
CORADS-5
CTSI(CT SEVERITY SCORE) with 17/25(severe)
with 68% lung involvement.


And RAPID ANTIGEN TEST is POSITIVE on 18.05.2021.

Past history:
He was diagnosed as diabetic 10 years back and hypertension 7 years back
And he is not a known case of Tuberculosis, Asthma, epilepsy
Personal History:
Appetite - loss of appetite
Diet - mixed
Bowl and bladder - regular
Sleep - adequate
Addictions - smoking - 3cigars/day since 40 years
chronic alcoholic since 20 years (last alcohol consumption- 5 days prior to hospitalization)
Allergies - no allergies
Family History:
There is no significant family history and no family contact of COVID-19.
GENERAL EXAMINATION:
Drowsy and arousable with altered sensorium [GCS - E2V2M5]
Moderately built and moderately nourished
Pallor- No pallor
Icterus - No Icterus
Cyanosis - No Cyanosis
Clubbing - No clubbing
Generalised Lymphadenopathy - No generalised lymphadenopathy
Pedal Edema - No pedal edema
VITALS :
At the time of admission:
Temperature - afebrile
Pulse - 114bpm
Blood Pressure - 110/70 mmHg
Respiratory Rate - 26cycles per minute
Spo2 - 77% on room air

On 1st day of hospitalization:
Temperature - afebrile
Pulse - 96bpm
Blood Pressure - 110/90 mmHg
Respiratory Rate - 20cycles per minute
Spo2 - 92% at 15 lit of O2

Temperature - afebrile
Pulse - 96bpm
Blood Pressure - 110/90 mmHg
Respiratory Rate - 24cycles per minute
Spo2 - 80% with 10 lit of O2

On 3rd day of hospitalization:
Temperature - afebrile
Pulse - 114bpm
Blood Pressure - 110/70 mmHg
Respiratory Rate - 26cycles per minute
Spo2 - 80% at room air & 90% with 10lit of O2
SYSTEMIC EXAMINATION:
CARDIOVASCULAR SYSTEM: S1 and S2 heart sounds heard. No murmers.
RESPIRATORY SYSTEM: Bilateral air entry present.
CENTRAL NERVOUS SYSTEM: altered sensorium with E2V2M5.
ABDOMEN: Soft and non-tender. Bowel sounds are heard. No organomegaly.
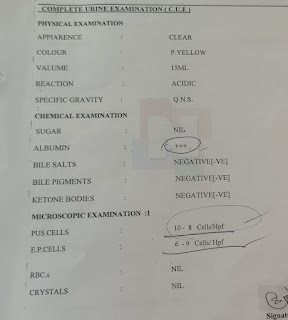
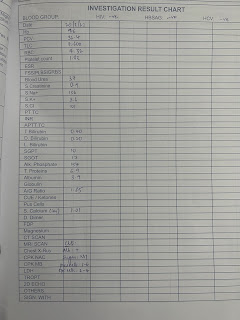
INVESTIGATIONS:
ABG : (on 7th day of symptoms)
pH - 7.28
pCO2 - 30.9mm Hg
pO2 - 33.5mm Hg
HCO3 - 14.1mmol/L
St.HCO3 - 14.8mmol/L
BEB - –11.2mmol/L
BEecf - –11.3mmol/L
TCO2 - 27.1 VOL
O2 Sat - 43.3%
O2 Count - 12.2 vol%

CBP :
HAEMOGLOBIN - 17gm/dl
TOTAL RBC COUNT - 5.2million/cu.mm
TOTAL WBC COUNT - 4,700 cells/cu.mm
NEUTROPHILS - 87%
LYMPHOCYTES - 10%
EOSINOPHILS - 01%
MONOCYTES - 02%
BASOPHILS - 00%
PLATELET COUNT - 1.5lakhs/cu.mm
SMEAR - NORMOCYTIC NORMOCHROMIC WITH RELATIVE NEUTROPHILIA

LFT :
Total Bilirubin - 2.56mg/dl
Direct Bilirubin - 0.63mg/dl
SGOT(AST) - 53IU/L
SGPT(ALT) - 20IU/L
ALKALINE PHOSPHATE - 204IU/L
TOTAL PROTEINS - 5.6gm/dl
ALBUMIN - 2.9gm/dl
A/G RATIO - 1.09

RFT -
UREA - 76mg/dl
CREATININE - 2.0mg/dl
URIC ACID - 5.9mg/dl
CALCIUM - 9.9mg/dl
PHOSPHORUS - 2.7mg/dl
SODIUM - 145mEq/L
POTASSIUM - 4.2mEq/L
CHLORIDE - 107mEq/L

D dimer - 830ng/ml

Serum LDH(Lactate dehydrogenase) - 591IU/L

CRP(C Reactive protein) - POSITIVE ( 0.6mg/dl)

RBS(Random blood sugar) - 279.5mg/dl

Diagnosis: VIRAL PNEUMONIA SECONDARY TO COVID-19
TREATMENT:
on 4th day of symptoms :
1. PRONE POSITIONING 2 HOURLY
2. Intermittent NIV [BIPAP] O2 Inhalation at 10-12lit/min
3. PROPPED UP POSTURE
4. Inj. DEXAMETHASONE 8mg /IV/TID
5. Inj. CLEXANE 60mg/SC/OD
6. Tab. PARACETAMOL 650mg/PO/TID
7. IVF - IONS with OPTINEURON and IORL at 100ml/hour
8. Monitor vitals at 4th hourly
9. GRBS checking at 8th hourly
10. Neb with DUOLIN at 6th hourly and BUDDCORT at 8th hourly
11. Tab. LIMCI 800mg/PO/OD
12. Tab. MVT/PO/OD
On 5th day of symptoms:
1. PRONE POSITIONING 2 HOURLY
2. Intermittent NIV [BIPAP] O2 Inhalation at 10-12lit/min
3. PROPPED UP POSTURE
4. Inj. DEXAMETHASONE 8mg /IV/TID
5. Inj. CLEXANE 60mg/SC/OD
6. Tab. PARACETAMOL 650mg/PO/TID
7. IVF - IONS with OPTINEURON and IORL at 100ml/hour
8. Monitor vitals at 4th hourly
9. GRBS checking at 8th hourly
10. Neb with DUOLIN at 6th hourly and BUDECORT at 8th hourly
11. Tab. LIMCEE 800mg/PO/OD
12. Tab. MVT/PO/OD
On 6th day of symptoms:
1. IV fluids NS and RL with THIAMINE and OPTINEURON
2. O2 Inhalation
3. DUOLIN BUDECORT Nebulization
4. Inj. CLEXANE 40mg BD
5. Inj, PANTOP 40 mg BD
6. Inj. DEXAMETHASONE 8mg IV OD
7. Tab. DOLO sos
8. Tab, LIMCEE OD
9. Tab, MVT OD
* CST and Inj. THIAMINE 100mg/TID
And Psychiatric opinion
On 7th day of symptoms:
1. IV Fluids NS and RL with THIAMINE and OPTINEURON
2. O2 Inhalation
3. DUOLIN BUDECORT Nebulization
4. Inj. CLEXANE 40mg IV OD
5. Tab. PANTOP 40mg OD
6. Tab. LIMCEE OD
7, Tab. MVT OD
* CST and Planning for NCCT Brain and if required intubation
Patient died on the 7th day of symptoms at 7pm.
DEATH SUMMARY:
This is a 65 years male patient admitted on 18.05.2021 with complaints of fever since 4 days and RAT for COVID-19 NEGATIVE and on 18.05.2021 HRCT CHEST SHOWED CORADS 5 with CTSI 17/25, diagnosed with viral pneumonia secondary to COVID-19. He was treated conservatively. This is a case of 65 years old male with complaints of fever since 4 days,loss of appetite on 18.05.2021, with the above complaints and his saturations were 77% on RA. He was on conservative treatment. Patient was in altered sensorium since admission for which psychiatry consultation taken and advise followed. Since 21.05.2021, 6:00pm suddenly saturations started falling down and patient became unresponsive immediately CPR started as per AHA guidelines but patient could not be revived. ECG showed no electrical activity and death declared at 7:00pm on 21.05.2021
Immediate cause: TYPE 2 RESPIRATORY FAILURE
Antecedent cause: VIRAL PNEUMONIA SECONDARY TO COVID-19 INFECTION
KEY POINTS:
65 years old male- chronic alcoholic and chronic smoker
Viral pneumonia secondary to COVID-19
Elevated liver enzymes and urea and creatinine.
Decreased pO2 and pCO2 in ABG.
Probable Questions:
1. What was the cause of altered sensorium?
2. What was the cause of death?
3. Can there was multiple organ failure due to covid-19?
Comments
Post a Comment