50 YEARS OLD MALE WITH WEAKNESS OF RIGHT UPPER LIKB AND LOWER LIMB
This is an online E-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient centered online learning portfolio and your valuable comments on comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Presenting complaints:
Patient came with the cheif complaints of weakness of right upper and lower limb since yesterday morning (04:00am) slurring of speech and deviation of mouth to left since yesterday morning.
HISTORY OF PRESENT ILLNESS:
patient was apparently asymptomatic 1 month back and then developed giddiness followed by. Fall and was diagnosed to be hypertension and used medication for 20 days and stopped 10 days ago. Asymptomatic till yesterday morning and noticed weakness of right upper and lower limb while trying to go to washroom associated with deviation of mouth to left and slurring of speech.no h/o difficulty in swallowing and giddiness.





PAST HISTORY:
known case of hypertension since 1 month (stopped medication 10 days ago). N/k/c/o DM, htn, CAD, thyroid, tb, ba
PERSONAL HISTORY:
factory employee by occupation addictions: chronic alcoholic since 20 years stopped for 1 month last binge 2 days ago
GENERAL PHYSICAL EXAMINATION:
Patient is conscious coherent and cooperative
No signs of pallor, icterus, cyanosis, clubbing, generalised lymphadenopathy
VITALS:
TEMPERATURE:98.6F
PULSE RATE:60bpm
RESPIRATORY RATE:14cpm
BLOOD PRESSURE: 140/80 mm Hg
SPO2:98% @ Room air
GRBS:149mg/dl
SYSTEMIC EXAMINATION:
CARDIOVASCULAR SYSTEM:
S1 and S2 Heard. No murmurs
RESPIRATORY SYSTEM:
NVBS HEARD. BAE PRESENT
CENTRAL NERVOUS SYSTEM:
Higher mental functions :-
Patient is conscious ,coherent and cooperative
Speech : slurred
No signs of meningeal irritation like neck stiffness and kernigs sign
Cranial nerves :- left sided deviation of mouth
Sensory system :-
Sensation right left
Touch felt felt
Pressure felt felt
Pain
-superficial felt felt
-deep felt felt
Proprioception
-joint position ✔ ✔
-joint movement ✔ ✔
Temperature felt felt
Vibration felt felt
Stereognosis ✔ ✔
Motor system
Right. Left
BULK
Upper limbs. N N
Lower limbs N N
TONE
Upper limbs. Increased Normal
Lower limbs. Increased Normal
POWER
Upper limbs. 3/5 5/5
Lower limbs 0/5 5/5
Reflexes :
Right. Left
Biceps. 3+ 3+
Triceps. 3+ 3+
Supinator 3+. 3+
Knee. 3+ 3+
Ankle. Extensor. Extensor
ROMBERGS sign : couldn't be elicited
No nystagmus
Dysdiadokinesia absent
No signs suggestive of cerebellar dysfunction
Gait: couldn't walk
PER ABDOMEN:
SOFT. NON TENDER.
NO ORGANOMEGALY
INVESTIGATIONS:
MRI BRAIN:

ACUTE INFARCT IN POSTERIOR LIMB OF LEFT INTERNAL CAPSULE
OLD LACUNAR INFARCT IN LEFT SIDE OF PONS
FEW MICROHEMORRHAGES IN BILATERAL CEREBRAL HEMISPHERES
MR ANGIOGRAM NORMAL
CHEST X RAY:

ELECTROCARDIOGRAPHY:

Serology:
HCV : non reactive
HIV: NON REACTIVE
RBS: 109mg/dl
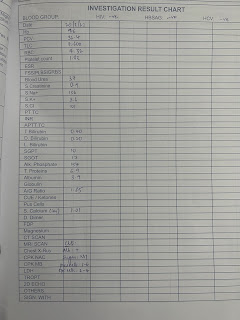
RFT:
Urea: 19mg/dl
Serum. Creatinine: 1.1mg/dl
S. Na+: 141 mEq/L
S. K+:. 3.7 mEq/L
S. Cl-: 1.02 mmol/L
FASTING BLOOD SUGAR: 114mg/dl
TFT:

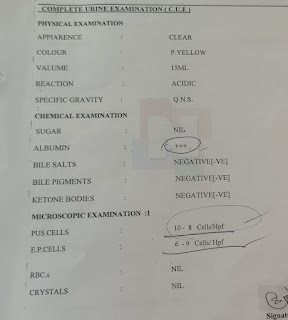
CUE:

HEMOGRAM:

LFT:

ULTRASOUND: NO SONOLOGICAL ABNORMALITY DETECTED
2DECHOCARDIOGRAPHY:
HEMOGRAM:
LIVER FUNCTION TEST:
RENAL FUNCTION TEST:
PROVISIONAL DIAGNOSIS:
CVA WITH RIGHT HEMIPARESIS WITH ? MCA STROKE
TREATMENT:
1. TAB. ECOSPRIN 150 MG PO/STAT
2. TAB. CLOPITAB 150 MG PO/STAT
3. TAB. ATORVAS 80 MG PO/STAT
4. PHYSIOTHERAPY OF UPPER AND LOWER LIMB
5. I/O CHARTING
6. VITALS MONITORING
7. INJ. OPTINEURON IN 1 AMP IN 500ML NS IV/OD
Comments
Post a Comment