GENERAL MEDICINE PREFINAL CASE
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs".
This E log book also reflects my patient-centered online learning portfolio and your valuable comments on comment box is welcome.
Name: KASTURI VIJAY KUMAR
Roll no: 56
CHEIF COMPLAINTS:
65 years old female from rural nalgonda came with cheif complaints of fever since 10 days, shortness of breathe since 2 days
HISTORY OF PRESENT ILLNESS:
The patient was apparently in her normal state of health 4 months ago.
She developed fever which was insidious in onset, intermittent in nature which was relieved on medication associated with generalised weakness
She also complaints of a chest pain on exertion
She also complains of shortness of breath grade 3 MMRC since 3 days. Associated with cough with expectoration (white sputum)
Yesterday she had a similar episode of fever of high grade with chills and rigors , weakness..which did not subside on medication
PAST HISTORY:
Known case of diabetes and hypertension from 10 years
Not a known case of tuberculosis, asthma, epilepsy, thyroid
Surgery for breast lump 5 months back
Underwent hysterectomy 15 years back
PERSONAL HISTORY:
Appetite: reduced since 1 year
Diet: mixed
Sleep: Adequate
Bowel and bladder : regular
Sleep: Adequate
Addictions: nil
Allergies: nil
FAMILY HISTORY: insignificant
GENERAL PHYSICAL EXAMINATION
Conscious coherent cooperative
Moderately built and Moderately nourished
Pallor: present


Icterus: no icterus
Cyanosis: no cyanosis
Clubbing: no clubbing
Generalised Lymphadenopathy: no generalised Lymphadenopathy
Pedal edema : no pedal edema
VITALS:
Temperature: febrile 103°F (101°F @ admission)

Pulse rate: 56 bpm(108bpm @ admission)
Respiratory rate: 18cpm(36cpm @ admission)
Blood pressure: 100/60mm Hg (140/80mm Hg @ admission)
SpO2: 97% at room air
GRBS: 96mg/dl
SYSTEMIC EXAMINATION:
RESPIRATORY SYSTEM:
UPPER RESPIRATORY TRACT:
Normal
LOWER RESPIRATORY TRACT:
Inspection:
Chest is bilaterally symmetrical
The trachea appears to be in centre
Apical impulse is not appreciated
Chest movements appears to be reduced on left side
No dilated veins, scars or sinuses are seen
Palpation-
Trachea is felt in midline
Movements Decresed on left side
Apical impulse is felt in the fifth intercostal space 1cm lateral to mid clavicular line
Tactile vocal fremitus- increased at left inframammary area
Percussion-
Left inframammary - dull note
Auscultation-
Normal vesicular breath sounds are heard
Fine crepts in left inframammary area, left infraaxillary area, infraclavicular area, infrascapular area
CARDIOVASCULAR SYSTEM:
First and second hard sounds heard. No murmurs.
CENTRAL NERVOUS SYSTEM:
Higher mental functions normal
No focal neurological deficit
Meningeal signs: absent
PER ABDOMEN:
Soft non tender
No organomegaly
INVESTIGATIONS:
ABG:
pH : 7.4
pCO2: 20.1
pO2: 76.1
HCO3: 13.3
Serum HCO3: 16.9
02 Saturation: 96%
HEMOGRAM:
Hemoglobin: 8.0g/dl
Total Leukocyte count: 21600/mm³
Platelets: 4 37 lakhs/mm³
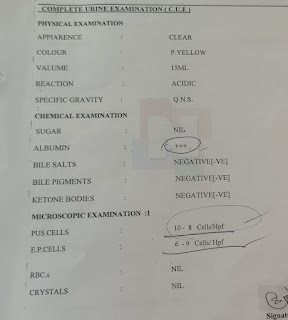
COMPLETE URINE EXAMINATION:
Albumin: positive
Sugar: nil
Pus cells: 4-5
Epithelial cells- 3-4
malaria: negative
RBS: 190mg/dl
Serum urea: 79
serum uruc acid: 7.4
serum creatinine: 2.3
Serum electrolytes:
Na+ : 134
K+ : 4
Cl- : 97
Ca+2: 9.6
LIVER FUNCTION TESTS:
Total bilirubin: 0.41
direct bilirubin: 0.13
AST: 29
ALT: 14
ALP: 166
Total protein: 5.7
Albumin: 2.31
Albumin: Globulin ratio: 0 68
CHEST X RAY:

ELECTROCARDIOGRAPHY:


TREATMENT:
1. IVF BS/RL 100ml/hour
2. Inj. PANTOP 40mg IV OD
3. SYRUP. ASCORYL-LS 100ml PO BD
4. O2 INHALATION
5. INJ. PIPTAZ
6. TAB. DOLO 650mg TID
7. INJ. NEOMOL 1mg IV NS
8. TEMPERATURE CHARTING 4TH HOURLY
9. GRBS 6TH HOURLY
10. INJ. HAI SC


Comments
Post a Comment