40 YEARS OLD MALE WITH DENGUE FEVER WITH LEFT SIDED PLEURAL EFFUSION WITH GLOMERULONEPHRITIS
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs".
This E log book also reflects my patient-centered online learning portfolio and your valuable comments on comment box is welcome.
MEDICINE CASE DISCUSSION:
I've been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
VIEW OF THE CASE:
A 40 years old male, Farmer by occupation, resident of nalgondacame with the cheif complaints of
Fever from 4 days
Cough from 3 days
blood in sputum from 3 days
red colored urine from 2 days
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 4 days ago, then he developed
Fever: duration- from 4 days,onset- insidious, grade- mild, intermittent, more during night time, with chills and associated with profuse sweating(clothes became wet). Subsided on taking medications. No history of Headache and vomitings.
Cough: duration- from 3 days, type- wet type, no postural variationProductive cough
Blood in sputum- duration- from 3 days, clots - present, associated with cough, no food particles, no epistaxis, no hematochezia,
Red colored urine : duration-from 2 days, associated with bilateral loin pain
No history of sorethroat, loss of consciousness, perioral surgeries, repeated choking episodes, joint pains, urgency,hesitancy, frequency
PAST HISTORY:
Similar complaints 10 days back and received medications from rural medical practitioner and releived from symptoms.
Not a known case of diabetes, hypertension, tuberculosis, asthma, epilepsy, thyroid disorder.
PERSONAL HISTORY:
Appetite- normal
Diet- mixed
Bowel and bladder habits- regular
Sleep- adequate
Addictions:
Alcohol- whisky- 180 ml twice weekly from 30 years
Smoking- 1 pack(20 beedis) per day since 30 years
Smoking index= 20×30= 600 - heavy smoker
Allergies- no allergies
FAMILY HISTORY:
Insignificant
GENERAL PHYSICAL EXAMINATION:
Patient is conscious, coherent, cooperative
Moderately built and moderately nourished
Comfortably seated
Pallor- no pallor
Icterus-no icterus
Cyanosis- no cyanosis
Clubbing- no clubbing
Generalised lymphadenopathy-no generalised lymphadenopathy
Pedal edema- no pedal edema
JVP-
VITALS:
On 26.09.2021
Temperature: febrile (99.5°F)
Pulse rate: 88 bpm
Respiratory Rate:
Blood Pressure: 110/90 mm Hg
On 27.09.2021
Temperature: febrile (101.5°F)
Pulse rate: 75 bpm
Respiratory Rate: 20 cycles/min
Blood Pressure: 80/60 mm Hg
On 28.09.2021
Temperature: afebrile (98.5°F)
Pulse rate: 78 bpm
Respiratory Rate: 18 cycles per minute
Blood Pressure: 110/70 mm Hg
On 29.09.2021
Temperature: afebrile (98.5°F)
Pulse rate: 80 bpm
Respiratory Rate: 18 cycles/minute
Blood Pressure: 110/80 mm Hg
FEVER CHART:

SYSTEMIC EXAMINATION:
CARDIOVASCULAR SYSTEM:
First and second heart sounds heard and no murmurs.
CENTRAL NERVOUS SYSTEM:
Higher motor functions intact
PER ABDOMEN EXAMINATION:
Non tender, bowel sounds heard.
RESPIRATORY SYSTEM:
Bilateral inspiratory and Expiratory wheeze in all lung fields
1. UPPER RESPIRATORY TRACT:
NOSE:
alae- normal
Nasi- normal
Septum- Normal
Polyps-absent
ORAL CAVITY:
teeth- blackish with poor dental hygiene
Gums- pigmented
Pharynx- normal
Sinus tenderness- absent
2. EXAMINATION OF CHEST:
INSPECTION:
- Shape of the chest- symmetrical
- Tracheal position- Central
- Apical impulse- seen
- Chest movements- Respiratory Rate- 20 cycles/min , type-abdominothoracic , rhythm- regular, intercostal indrawing- absent
- Skin over the chest- enorged veins- absent, sinuses- absent, subcutaneous nodules- absent, intercostal scars- absent, intercostal swellings-absent
- Trail sign- absent
- Temperature - no rise of temperature
- Tenderness- non tender
- All inspectory findings- confirmed
- Expansion of chest- symmetrical
- Tactile vocal fremitus- decreased on left side
- Bony tenderness- absent
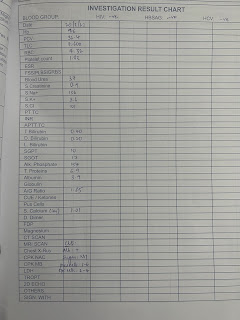
INVESTIGATIONS:
ELECTROCARDIOGRAPHY:

ULTRASONOGRAPHY:

HEMOGRAM:

HRCT- CHEST

CHEST X RAY:
On 27.09.2021

On 29.09.2021

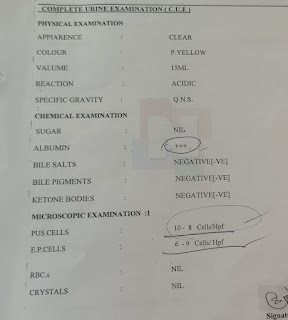
COMPLETE URINE EXAMINATION:
Blood urea: 60
Serum creatinine: 1.4
Na+:140mEql/L
K+: 4.1mEql/L
Cl–: 96mEql/L
Urine protein: 11.0
Urine creatinine: 38.2
Urine protein : creatinine - 0.28
ERYTHROCYTE SEDIMENTATION RATE: 90
MALARIAL PARASITE - NEGATIVE
LIVER FUNCTION TEST:
Total bilirubin: 1.08
Direct Bilirubin: 0.27
AST: 56
ALT: 19
ALP: 154
Albumin- 2.6
Total protein: 4.3
Albumin: globulin- 1.02
NS1 : POSITIVE
COMPLETE BLOOD PICTURE:
Hemoglobin: 14.4g/dl
Total Leukocyte count- 11500
Neutrophils- 80%
Lymphocytes- 15%
Monocytes- 03%
Eosinophils- 02%
PCV- 39.0
MCV- 85.2
MCH- 31.4
MCHC- 36.9
RDW CV- 11.8
RDW SD- 37.2
RBC- 4,53
Neutrophils- 78%
Lymphocytes- 14%
Eosinophils-1%
Basophils- 0%
PCV- 36.9
MCV- 84.2
MCH-31.3
MCHC-37.1
RDW-CU: 11.7
RDW-SD: 19.1
RBC- 4.38
Platelets- 40000
PROTHROMBIN TIME: 18
ApTT: 36
INR: 1.3
DIAGNOSIS:
DENGUE FEVER WITH LEFT SIDED PLEURAL EFFUSION WITH GLOMERULONEOHRITIS
TREATMENT:
On 26.09.2021
1. INTRAVENOUS FLUIDS- NS/RL
2. Inj. PAN
3. NEBULIZATION WITH BUDECORT DUOLIN
On 27.09.2021
1. INTRAVENOUS FLUIDS- NS/RL
2. Tab. AUGMENTIN
3. Tab. PAN
4. Syrup. ASCORIL
5. Inj. NEOMOL
6. NEBULIZATION WITH BUDECORT DUOLIN
On 28.09.2021
1. INTRAVENOUS FLUIDS-NS/RL
2. Inj. CEFTRIAXONE
3. Inj. DOXYCYCLINE
4. Inj. PAN
5. Inj. NEOMOL
6. Syrup. ASCORIL
7. NEBULIZATION WITH BUDECORT DUOLIN
On 29.09.2021
1. INTRAVENOUS FLUIDS- NS/RL
2. Inj. CEFTRIAXONE
3. Inj. DOXYCYCLINE
4. Inj. NEOMOL
5. Syrup. ASCORIL
6. NEBULIZATION WITH BUDECORT DUOLIN
Comments
Post a Comment